Abstract
Primary synovial chondromatosis is a rare benign monoarticular disorder characterized by cartilaginous metaplasia of the synovium with formation of multiple intra-articular nodules and loose bodies. Although the knee and hip are most commonly involved, ankle localization remains exceptional and may lead to delayed diagnosis because of nonspecific clinical manifestations.
We report the case of a 36-year-old woman presenting with a one-year history of progressive mechanical pain of the right ankle without restriction of motion. Clinical examination revealed mild ankle swelling, tenderness over the medial and lateral malleoli, a positive anterior drawer test, and signs of anterior impingement. Laboratory investigations were unremarkable. Plain radiographs demonstrated multiple calcified loose bodies around the tibiotalar joint associated with mild osseous erosions. Magnetic resonance imaging (MRI) revealed diffuse synovial thickening with numerous intra-articular nodules extending into the tibiotalar joint, distal tibiofibular recess, subtalar joint, and lateral malleolar region. The nodules showed low signal intensity on T1-weighted images, predominantly high signal intensity on proton density fat-suppressed sequences, and punctate signal voids corresponding to mineralized foci.
The patient underwent open synovectomy with complete removal of the loose bodies. Histopathological examination confirmed primary synovial chondromatosis. Postoperative recovery was uneventful, with favorable clinical evolution.
This case highlights the importance of considering primary synovial chondromatosis in the differential diagnosis of chronic ankle pain. MRI plays a pivotal role in identifying non-mineralized nodules, assessing disease extent, guiding surgical management, and differentiating this entity from other proliferative synovial disorders.
Keywords: Synovial chondromatosis; Ankle joint; Magnetic resonance imaging; Loose bodies; Synovial proliferative disorders
We report the case of a 36-year-old woman presenting with a one-year history of progressive mechanical pain of the right ankle without restriction of motion. Clinical examination revealed mild ankle swelling, tenderness over the medial and lateral malleoli, a positive anterior drawer test, and signs of anterior impingement. Laboratory investigations were unremarkable. Plain radiographs demonstrated multiple calcified loose bodies around the tibiotalar joint associated with mild osseous erosions. Magnetic resonance imaging (MRI) revealed diffuse synovial thickening with numerous intra-articular nodules extending into the tibiotalar joint, distal tibiofibular recess, subtalar joint, and lateral malleolar region. The nodules showed low signal intensity on T1-weighted images, predominantly high signal intensity on proton density fat-suppressed sequences, and punctate signal voids corresponding to mineralized foci.
The patient underwent open synovectomy with complete removal of the loose bodies. Histopathological examination confirmed primary synovial chondromatosis. Postoperative recovery was uneventful, with favorable clinical evolution.
This case highlights the importance of considering primary synovial chondromatosis in the differential diagnosis of chronic ankle pain. MRI plays a pivotal role in identifying non-mineralized nodules, assessing disease extent, guiding surgical management, and differentiating this entity from other proliferative synovial disorders.
Keywords: Synovial chondromatosis; Ankle joint; Magnetic resonance imaging; Loose bodies; Synovial proliferative disorders
Introduction
Primary synovial chondromatosis is a rare benign proliferative disorder characterized by cartilaginous metaplasia of the synovial membrane, resulting in the formation of multiple intra-articular cartilaginous nodules and loose bodies [1]. Over time, these nodules may calcify or ossify, leading to the term synovial osteochondromatosis. The condition most frequently affects large weight-bearing joints, particularly the knee, followed by the hip, shoulder, and elbow [2].
Ankle involvement is uncommon and represents only a small proportion of reported cases in the literature [2]. Because of its rarity and nonspecific clinical presentation, diagnosis may be delayed or initially mistaken for more common causes of chronic ankle pain, including ligamentous instability, impingement syndromes, or inflammatory arthropathies.
Imaging plays a central role in diagnosis, particularly magnetic resonance imaging (MRI), which enables detection of both mineralized and non-mineralized nodules, evaluation of synovial proliferation, assessment of extra-articular extension, and preoperative planning.
We report a rare case of primary synovial chondromatosis of the ankle in a 36-year-old woman and discuss the clinical presentation, imaging findings, differential diagnosis, histopathological features, and therapeutic management in light of the current literature.
Ankle involvement is uncommon and represents only a small proportion of reported cases in the literature [2]. Because of its rarity and nonspecific clinical presentation, diagnosis may be delayed or initially mistaken for more common causes of chronic ankle pain, including ligamentous instability, impingement syndromes, or inflammatory arthropathies.
Imaging plays a central role in diagnosis, particularly magnetic resonance imaging (MRI), which enables detection of both mineralized and non-mineralized nodules, evaluation of synovial proliferation, assessment of extra-articular extension, and preoperative planning.
We report a rare case of primary synovial chondromatosis of the ankle in a 36-year-old woman and discuss the clinical presentation, imaging findings, differential diagnosis, histopathological features, and therapeutic management in light of the current literature.
Case Presentation
A 36-year-old woman presented with a one-year history of progressively worsening mechanical pain involving the right ankle. The pain was exacerbated by walking and prolonged standing, without associated inflammatory symptoms or constitutional manifestations. There was no history of trauma, instability, locking, or prior ankle surgery.
Physical examination demonstrated mild ankle swelling without erythema or cutaneous inflammatory changes. Palpation elicited tenderness over both malleoli and along the tibiotalar joint line. Range of motion was preserved. Stability testing revealed a positive anterior drawer test, suggesting increased anterior translation of the talus, while forced dorsiflexion reproduced pain consistent with anterior impingement. Neurovascular examination was normal.
Laboratory investigations, including complete blood count, erythrocyte sedimentation rate, C-reactive protein, and metabolic parameters, were within normal limits, with no evidence of inflammatory or infectious disease.
Plain radiographs of the right ankle demonstrated multiple rounded and ovoid calcified bodies projected predominantly over the anterior aspect of the tibiotalar joint, associated with mild adjacent soft tissue swelling and subtle erosive changes involving the distal tibia and fibula. The ankle mortise and subtalar joint spaces remained preserved (Figure 1).

Subsequent MRI revealed diffuse synovial thickening associated with numerous nodular intra-articular lesions extending into the tibiotalar joint, distal tibiofibular recess, subtalar joint, and along the lateral malleolar region. The nodules demonstrated low signal intensity on T1-weighted images and predominantly high signal intensity on proton density fat-suppressed sequences, with heterogeneous post-contrast enhancement. Several nodules contained punctate foci of signal void corresponding to calcifications identified on radiographs. Mild pressure erosions of adjacent osseous structures were also noted, without bone marrow invasion (Figure 2).
Based on the clinical and imaging findings, primary synovial chondromatosis was strongly suspected.
The patient underwent open surgical synovectomy through an anterior ankle approach. Intraoperatively, multiple cartilaginous nodules and proliferative synovial tissue were identified within the tibiotalar joint and adjacent recesses. Complete excision of the pathological synovium and removal of all visible loose bodies were performed.
Histopathological examination revealed lobulated cartilaginous nodules arising from the synovium and separated by fibrous septa. The nodules were composed of chondrocytes embedded within a myxochondroid matrix without significant cytologic atypia, mitotic activity, or necrosis, consistent with primary synovial chondromatosis.
Postoperative recovery was uneventful. The patient underwent standard rehabilitation with progressive improvement in pain and functional symptoms.
Physical examination demonstrated mild ankle swelling without erythema or cutaneous inflammatory changes. Palpation elicited tenderness over both malleoli and along the tibiotalar joint line. Range of motion was preserved. Stability testing revealed a positive anterior drawer test, suggesting increased anterior translation of the talus, while forced dorsiflexion reproduced pain consistent with anterior impingement. Neurovascular examination was normal.
Laboratory investigations, including complete blood count, erythrocyte sedimentation rate, C-reactive protein, and metabolic parameters, were within normal limits, with no evidence of inflammatory or infectious disease.
Plain radiographs of the right ankle demonstrated multiple rounded and ovoid calcified bodies projected predominantly over the anterior aspect of the tibiotalar joint, associated with mild adjacent soft tissue swelling and subtle erosive changes involving the distal tibia and fibula. The ankle mortise and subtalar joint spaces remained preserved (Figure 1).
Figure 1
Figure 1: Anteroposterior (A) and lateral (B) radiographs of the right ankle demonstrating multiple rounded and ovoid calcified bodies projected over the anterior aspect of the tibiotalar joint, consistent with mineralized intra-articular loose bodies (white arrows).
×
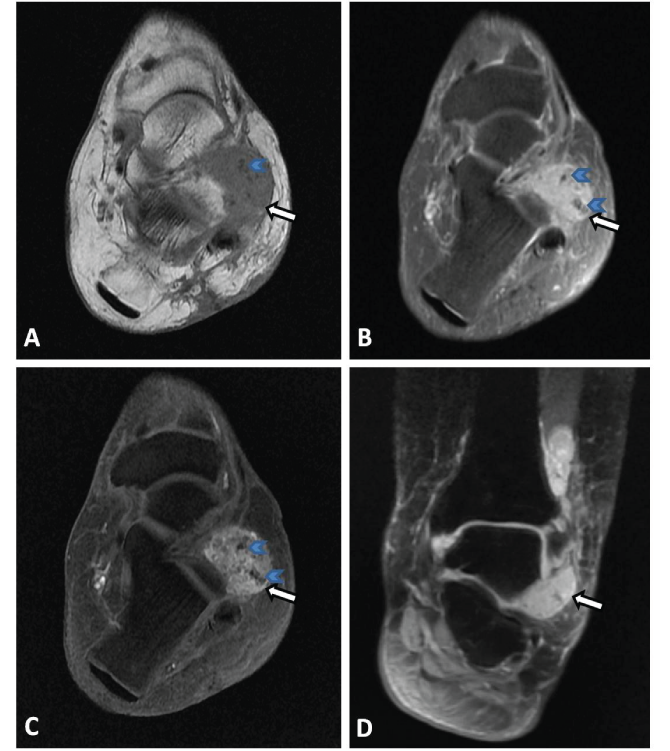
Figure 2
Figure 2: Axial T1-weighted (A), axial proton density fat-suppressed (B), axial post-contrast (C), and coronal proton density fat-suppressed (D) MR images demonstrating diffuse synovial thickening with multiple nodular lesions extending into the tibiotalar joint, distal tibiofibular recess, subtalar joint, and along the lateral malleolar region (white arrows). The nodules demonstrate low signal intensity on T1-weighted images and predominantly high signal intensity on proton density fat-suppressed sequences, with post-contrast enhancement. Several nodules contain punctate foci of signal void corresponding to calcified components (blue arrowheads).
×
The patient underwent open surgical synovectomy through an anterior ankle approach. Intraoperatively, multiple cartilaginous nodules and proliferative synovial tissue were identified within the tibiotalar joint and adjacent recesses. Complete excision of the pathological synovium and removal of all visible loose bodies were performed.
Histopathological examination revealed lobulated cartilaginous nodules arising from the synovium and separated by fibrous septa. The nodules were composed of chondrocytes embedded within a myxochondroid matrix without significant cytologic atypia, mitotic activity, or necrosis, consistent with primary synovial chondromatosis.
Postoperative recovery was uneventful. The patient underwent standard rehabilitation with progressive improvement in pain and functional symptoms.
Discussion
Primary synovial chondromatosis is an uncommon benign neoplastic-like disorder resulting from cartilaginous metaplasia of the synovial membrane [1]. The disease predominantly affects adults between the third and fifth decades of life and demonstrates a male predominance, with reported male-to-female ratios reaching 2–3:1 [2]. The knee accounts for approximately 60–70% of cases, whereas ankle involvement remains rare [2].
Primary synovial chondromatosis should be distinguished from secondary synovial chondromatosis. Primary disease arises from idiopathic synovial metaplasia and is characterized by numerous nodules of relatively uniform size associated with active synovial proliferation. In contrast, secondary synovial chondromatosis occurs in the setting of preexisting joint abnormalities such as osteoarthritis, trauma, osteochondritis dissecans, or neuropathic arthropathy. Secondary forms usually demonstrate fewer loose bodies with more variable size and less prominent synovial proliferation [3].
The pathogenesis of primary synovial chondromatosis remains incompletely understood. Synovial cells undergo cartilaginous metaplasia, producing nodules that may detach into the joint cavity and continue to grow under the influence of synovial fluid nutrition. Progressive calcification or ossification may subsequently occur.
Milgram described three histopathological phases of the disease [1]: an initial active intrasynovial phase without loose bodies, a transitional phase with active synovial proliferation and loose body formation, and a late phase characterized predominantly by multiple detached loose bodies with limited residual synovial activity.
Clinically, patients usually present with chronic monoarticular pain, swelling, stiffness, limitation of motion, and occasionally mechanical symptoms such as locking or clicking due to mobile intra-articular bodies [1]. However, symptoms are often nonspecific and may mimic more common ankle disorders, contributing to delayed diagnosis. In the present case, the absence of marked inflammatory signs or limitation of motion initially suggested ligamentous instability or impingement syndrome.
Imaging plays a pivotal role in diagnosis and treatment planning. Conventional radiography may demonstrate multiple calcified or ossified loose bodies, typically showing characteristic “ring-and-arc” chondroid mineralization patterns [3]. Calcifications are reported in approximately 70–95% of cases depending on disease stage and degree of ossification.
MRI is particularly valuable in detecting non-mineralized cartilaginous nodules and evaluating the extent of synovial involvement. Typical MRI findings include lobulated intra-articular nodules demonstrating low-to-intermediate signal intensity on T1-weighted images and high signal intensity on T2-weighted or proton density fat-suppressed sequences. Foci of low signal intensity or signal void correspond to calcified or ossified components [4]. Synovial thickening and variable post-contrast enhancement are commonly observed. MRI is also useful for assessing extra-articular extension, erosive changes, and adjacent soft tissue involvement.
Computed tomography may complement MRI by more accurately depicting mineralized loose bodies and subtle osseous erosions, particularly in anatomically complex joints such as the ankle.
The principal radiological differential diagnosis is tenosynovial giant cell tumor (TSGCT), also referred to as pigmented villonodular synovitis (PVNS). Unlike primary synovial chondromatosis, TSGCT typically demonstrates diffuse low signal intensity on both T1- and T2-weighted images due to hemosiderin deposition, often associated with blooming artifacts on gradient-echo sequences [5]. Calcified loose bodies are uncommon in TSGCT, whereas mineralized nodules strongly favor synovial chondromatosis. Other differential diagnoses include osteoarthritis with secondary loose bodies, osteochondritis dissecans, lipoma arborescens, and, more rarely, synovial chondrosarcoma.
Lipoma arborescens usually presents as villous fatty synovial proliferation demonstrating high signal intensity on T1-weighted images with complete suppression on fat-saturated sequences and lacks calcified nodules. Osteoarthritis-related loose bodies are generally associated with advanced degenerative changes and fewer, irregular osteochondral fragments [6].
Histopathological examination remains essential for definitive diagnosis and exclusion of malignant transformation. Although rare, transformation of primary synovial chondromatosis into synovial chondrosarcoma has been reported [7]. Features suggestive of malignancy include aggressive bone destruction, bone marrow invasion, permeative growth pattern, marked cytologic atypia, and increased mitotic activity.
The standard treatment for symptomatic disease consists of surgical removal of loose bodies combined with partial or complete synovectomy when feasible [8]. Arthroscopic treatment has been successfully reported for ankle involvement and offers advantages including reduced postoperative morbidity and faster rehabilitation. However, open surgery may be preferable in extensive disease to facilitate complete excision of proliferative synovium and loose bodies.
Recurrence remains a recognized complication, with reported rates ranging from approximately 10% to 20% depending on the extent of synovectomy and completeness of excision [9]. Long-term clinical and imaging follow-up is therefore recommended.
Primary synovial chondromatosis should be distinguished from secondary synovial chondromatosis. Primary disease arises from idiopathic synovial metaplasia and is characterized by numerous nodules of relatively uniform size associated with active synovial proliferation. In contrast, secondary synovial chondromatosis occurs in the setting of preexisting joint abnormalities such as osteoarthritis, trauma, osteochondritis dissecans, or neuropathic arthropathy. Secondary forms usually demonstrate fewer loose bodies with more variable size and less prominent synovial proliferation [3].
The pathogenesis of primary synovial chondromatosis remains incompletely understood. Synovial cells undergo cartilaginous metaplasia, producing nodules that may detach into the joint cavity and continue to grow under the influence of synovial fluid nutrition. Progressive calcification or ossification may subsequently occur.
Milgram described three histopathological phases of the disease [1]: an initial active intrasynovial phase without loose bodies, a transitional phase with active synovial proliferation and loose body formation, and a late phase characterized predominantly by multiple detached loose bodies with limited residual synovial activity.
Clinically, patients usually present with chronic monoarticular pain, swelling, stiffness, limitation of motion, and occasionally mechanical symptoms such as locking or clicking due to mobile intra-articular bodies [1]. However, symptoms are often nonspecific and may mimic more common ankle disorders, contributing to delayed diagnosis. In the present case, the absence of marked inflammatory signs or limitation of motion initially suggested ligamentous instability or impingement syndrome.
Imaging plays a pivotal role in diagnosis and treatment planning. Conventional radiography may demonstrate multiple calcified or ossified loose bodies, typically showing characteristic “ring-and-arc” chondroid mineralization patterns [3]. Calcifications are reported in approximately 70–95% of cases depending on disease stage and degree of ossification.
MRI is particularly valuable in detecting non-mineralized cartilaginous nodules and evaluating the extent of synovial involvement. Typical MRI findings include lobulated intra-articular nodules demonstrating low-to-intermediate signal intensity on T1-weighted images and high signal intensity on T2-weighted or proton density fat-suppressed sequences. Foci of low signal intensity or signal void correspond to calcified or ossified components [4]. Synovial thickening and variable post-contrast enhancement are commonly observed. MRI is also useful for assessing extra-articular extension, erosive changes, and adjacent soft tissue involvement.
Computed tomography may complement MRI by more accurately depicting mineralized loose bodies and subtle osseous erosions, particularly in anatomically complex joints such as the ankle.
The principal radiological differential diagnosis is tenosynovial giant cell tumor (TSGCT), also referred to as pigmented villonodular synovitis (PVNS). Unlike primary synovial chondromatosis, TSGCT typically demonstrates diffuse low signal intensity on both T1- and T2-weighted images due to hemosiderin deposition, often associated with blooming artifacts on gradient-echo sequences [5]. Calcified loose bodies are uncommon in TSGCT, whereas mineralized nodules strongly favor synovial chondromatosis. Other differential diagnoses include osteoarthritis with secondary loose bodies, osteochondritis dissecans, lipoma arborescens, and, more rarely, synovial chondrosarcoma.
Lipoma arborescens usually presents as villous fatty synovial proliferation demonstrating high signal intensity on T1-weighted images with complete suppression on fat-saturated sequences and lacks calcified nodules. Osteoarthritis-related loose bodies are generally associated with advanced degenerative changes and fewer, irregular osteochondral fragments [6].
Histopathological examination remains essential for definitive diagnosis and exclusion of malignant transformation. Although rare, transformation of primary synovial chondromatosis into synovial chondrosarcoma has been reported [7]. Features suggestive of malignancy include aggressive bone destruction, bone marrow invasion, permeative growth pattern, marked cytologic atypia, and increased mitotic activity.
The standard treatment for symptomatic disease consists of surgical removal of loose bodies combined with partial or complete synovectomy when feasible [8]. Arthroscopic treatment has been successfully reported for ankle involvement and offers advantages including reduced postoperative morbidity and faster rehabilitation. However, open surgery may be preferable in extensive disease to facilitate complete excision of proliferative synovium and loose bodies.
Recurrence remains a recognized complication, with reported rates ranging from approximately 10% to 20% depending on the extent of synovectomy and completeness of excision [9]. Long-term clinical and imaging follow-up is therefore recommended.
Conclusion
Primary synovial chondromatosis of the ankle is an exceptionally rare cause of chronic ankle pain that may present with subtle and nonspecific clinical manifestations. Awareness of this entity is important to avoid delayed diagnosis, particularly in patients with persistent mechanical symptoms and preserved joint mobility.
Radiographs may reveal characteristic calcified loose bodies in advanced stages; however, MRI remains essential for detecting non-mineralized nodules, evaluating disease extent, assessing erosive changes, and differentiating synovial chondromatosis from other proliferative synovial disorders such as TSGCT/PVNS.
Complete surgical excision of loose bodies combined with synovectomy remains the cornerstone of treatment and may reduce the risk of recurrence. Histopathological confirmation is mandatory to establish the diagnosis and exclude malignant transformation.
Radiographs may reveal characteristic calcified loose bodies in advanced stages; however, MRI remains essential for detecting non-mineralized nodules, evaluating disease extent, assessing erosive changes, and differentiating synovial chondromatosis from other proliferative synovial disorders such as TSGCT/PVNS.
Complete surgical excision of loose bodies combined with synovectomy remains the cornerstone of treatment and may reduce the risk of recurrence. Histopathological confirmation is mandatory to establish the diagnosis and exclude malignant transformation.
Declarations
Conflict of Interest
The authors declare that there is no conflict of interest regarding the publication of this article.Informed Consent
Written informed consent was obtained from the patient for participation in this case report and for publication of any accompanying images.Ethical Approval
Ethical approval is not required at our institution for anonymous case reports.References
- Sedeek SM, Choudry Q, Garg S. Synovial chondromatosis of the ankle joint: clinical, radiological, and intraoperative findings. Case Rep Orthop. 2015; 2015: 359024.
- Kachuee MA, Mohseni I, Emtiazi N, Sharifi Y. Ankle synovial chondromatosis: clinical, radiological, and surgical findings: a case report. Radiol Case Rep. 2024; 19(8): 3227–3230.
- McKenzie G, Raby N, Ritchie D. A pictorial review of primary synovial osteochondromatosis. Eur Radiol. 2008; 18(11): 2662–2669.
- Murphey MD, et al. Chondroid tumors: review of imaging features and update on WHO classification. Curr Probl Diagn Radiol. 2023.
- Mohey N, Hassan TA. Feasibility of MRI in diagnosis and characterization of intra-articular synovial masses and mass-like lesions. Egypt J Radiol Nucl Med. 2020; 51: 19.
- Tsukamoto J, Fujisaki A, Futatsuya K, et al. Imaging findings of intra-articular tumor/tumor-like lesions based on pathologic correlation. Jpn J Radiol. 2025.
- Bertoni F, Unni KK, Beabout JW, Sim FH. Chondrosarcomas of the synovium. Cancer. 1991; 67(1): 155–162.
- Moorthy V, Tay KS, Koo K. Arthroscopic treatment of primary synovial chondromatosis of the ankle: a case report and review of literature. J Orthop Case Rep. 2020; 10(6): 54–59.
- Maurice H, Crone M, Watt I. Synovial chondromatosis. J Bone Joint Surg Br. 1988; 70(5): 807–811.